Brachial Plexus Injury
ANATOMY
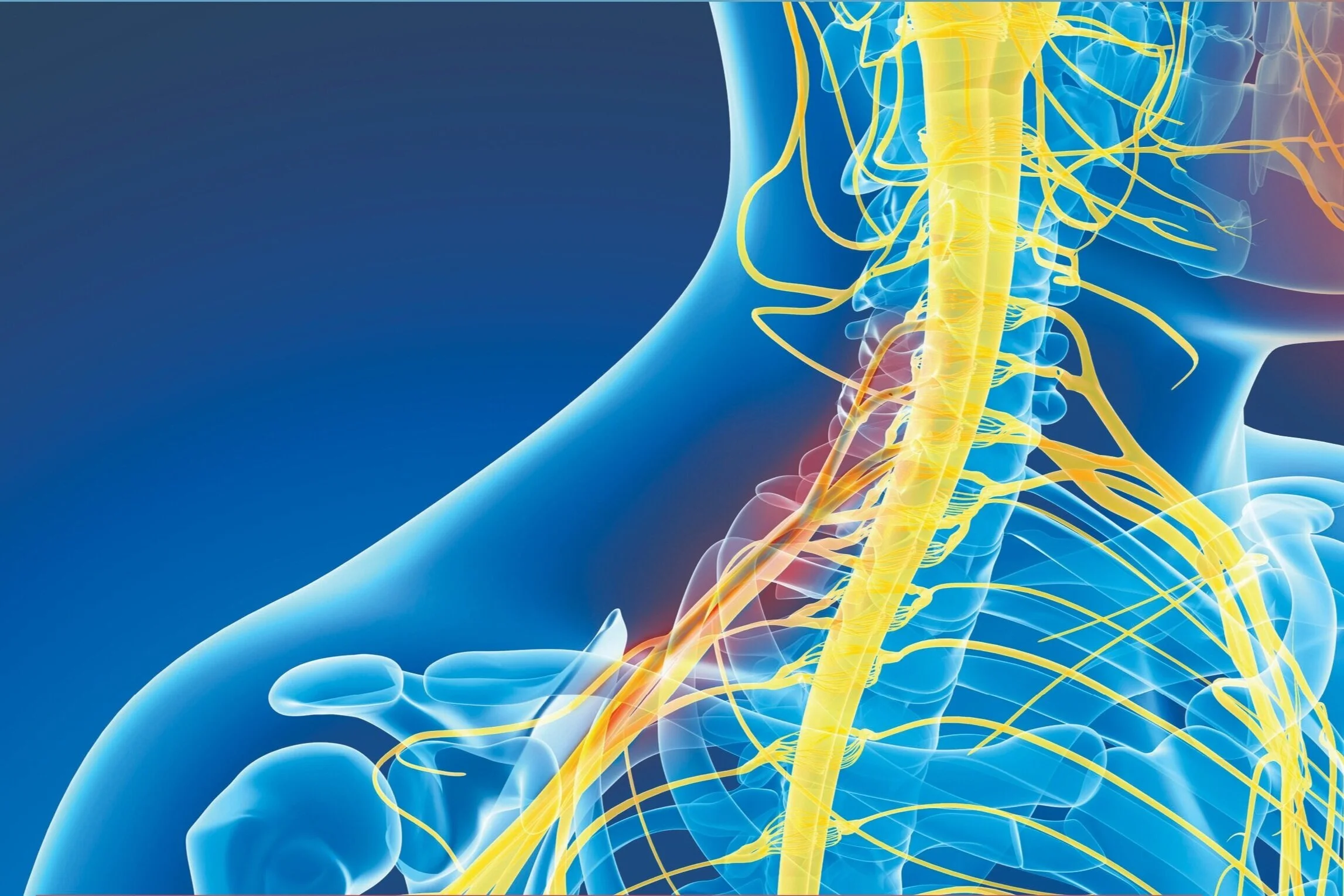
The brachial plexus is a complex network of nerves that extends from the spinal cord within the neck through the axilla (armpit) and supplies nerves to the chest, shoulder, and arm. These nerves control your shoulder, arm, wrist and hand, allowing you to raise your arm, type on your keyboard, or throw a baseball. The brachial plexus nerves are sensory, too. For instance, these nerves let you know that the pain you just grabbed with your hand is too hot to hold or that when you reach into your pocket you can distinguish a quarter from a nickel.
What Causes Brachial Plexus Injuries?
The brachial plexus can be injured in many different ways — but most commonly it is from a traumatic injury. The nerves may also be damaged by inflammatory disorders, cancer or radiation treatment. Sometimes, brachial plexus injuries happen to babies during childbirth.
The traumatic injuries in adults are most commonly from motorcycle, snowmobile, ATV, football or other high velocity high-energy impacts that pull the shoulder down while the head is pushed away. This same scenario can occur with a difficult childbirth – the shoulder is pulled down as the child passes through the birth canal and they can only be safely delivered by using significant force in this same trajectory.
Brachial plexus injuries may reduce or eliminate the communication between the spinal cord and the shoulder, arm, wrist, and hand. This may mean both loss of feeling and loss of use of your arm or hand or both. The severity of a brachial plexus injury varies. In some people, function and feeling return to normal over days to weeks. Others may have lifelong disabilities because they can't move or feel a part or all of the arm.
Brachial plexus injuries are categorized by which part of the plexus is injured and how severely it is injured. Nerves can be stretched and remain in continuity. Alternatively, they can be ruptured or severed. Occasionally, the nerve can actually be pulled directly out of the spinal cord. This is referred to as an avulsion injury.
Nerve injuries can be broadly categorized according to the Seddon Classification:
Neurapraxia The nerves are intact but not functioning. They can recover nicely if the compression has been relieved
Axonotmesis The wires within the nerve (axons) are actually severed and for recovery to take place they must grow back from the site of injury to the muscle and establish a new connection
Neurotmesis This refers to a severed nerve. The rupture described above is an example of a neurotmetic injury
Brachial Plexus Surgery - Partial Injuries
Upper plexus injury
Partial injuries most commonly occur in the upper part of the brachial plexus and result in paralysis of shoulder and elbow function. The arm is left hanging at the side, but hand function is usually preserved.
Lower plexus injury
More rarely, an injury can primarily affect the lower portion of the plexus and the hand will be disabled while the shoulder and biceps remain functional
Brachial Plexus Symptoms
Mild brachial plexus injuries typically feel like tingling and mild weakness in the arm, which will generally heal itself over time without surgical intervention. However, if there is more dramatic numbness and paralysis in the arm and/or hand, this signifies a more severe brachial plexus injury and it is critical you are seen by one of our paralysis specialists right away.
Diagnosis & Treatment Of A Brachial Plexus Injury
A brachial plexus injury is the most complex nerve injury to repair. Accurate diagnosis of the severity of the injury is crucial. It is important to determine whether the injury will recover with time or if surgery will be required in order to restore movement to the arm. Our specialist team provides a comprehensive approach in the diagnosis and management of severe brachial plexus injuries. In the event of a brachial plexus injury, our team uses a special form of magnetic resonance imaging (MRI) to determine:
exact location of the primary injury if there are ruptures
if there are avulsions (separations or detachments of the nerve root from the spinal cord)
if some of the nerves are more normal and healthy appearing and therefore more likely to recover in time.
Further confirmation of the type of injury and prediction of potential for recovery can be provided by neurophysiological studies, including electromyography (EMG) and nerve conduction studies (NCS). Using the information gathered from these tests, our team of specialists will develop a comprehensive plan to restore movement to your arm as quickly and as safely as possible. This may involve rehabilitation, Reconstructive Neurosurgery, or both. The earlier you undergo evaluation following your brachial plexus injury, the more treatment options are available to you to improve function.
Please don’t wait to see a brachial plexus specialist – call the Paralysis Center today to make your appointment.
Surgery For Brachial Plexus Injury
When the brachial plexus is completely injured, patients have no function at all in their extremity. They generally can neither feel nor move their arm. They often have severe pain, but not always. With these injuries, it is important to determine which nerves are scarred or torn, and which ones are avulsed (pulled out of the spinal cord). If nerves are avulsed, the surgeon can operate earlier instead of giving time for recovery, knowing that these injuries will not recover on their own. Nerves that are avulsed can be recovered using nerve transfers, or using another nerve that is connected to the spinal cord to repair the avulsed nerve. Nerves that are ruptured or scarred can often be repaired with nerve grafts.
These grafts are used to bypass the segment that is injured and allow the proximal nerve send its axons through the graft and back into the nerve beyond the injured segment. These axons should then make their way to the original destination to recover feeling and movement. Reconstructive surgery for complete brachial plexus injuries generally consists of a combination of nerve grafting and nerve transfer procedures. The treatment for each patient will be determined according to his or her individual condition. The surgical strategy is primarily determined by which nerves are available to be used in the reconstructive strategy.
Patients ideally undergo surgery within three to four months after their injury. In order to provide for the best recovery, it is often important that the patient receive physical therapy before the surgery to keep the joints mobile and to learn how to activate the nerves that will be transferred. After the surgery therapy becomes even more important for the patient to strengthen weak and recovering muscles and in order to learn to use the recovering muscles that are now run by different nerves in the case of nerve transfers.
For severe brachial plexus injuries, prompt surgery provides the most options for successful reconstruction. Without it, you may have fewer options and those options may involve bigger operations with longer hospitalizations. If you have a brachial plexus injury resulting in a lack of feeling, you must take special care when dealing with items that are hot or sharp or other objects that could harm you. When you have lost feeling to your arm and hand, you may not notice that you're hurt. Even an arm with no feeling may still experience pain.
Download Brachial Plexus Patient Guide
Schedule a Consult with the Paralysis Center today (844) 930-1001.
Tips to help you get the most from a visit to the Paralysis Center
Before your visit, write down questions you want answered.
Bring someone with you to help you ask questions and remember what your Specialist tells you.
At the visit, write down the name of your diagnosis, and any new medicines, treatments, or tests. Also write down any new instructions your specialist gives you.
Know why a new medicine or treatment is prescribed, and how it will help you. Also know what the side effects are.
Ask if your condition can be treated in other ways.
Know why a test or procedure is recommended and what the results could mean.
Know what to expect if you do not take the medicine or have the test or procedure.
If you have a follow-up appointment, write down the date, time, and purpose for that visit.
Know how you can contact your Paralysis Specialist if you have questions.